


BN#47 How to Use The Compassionate Mind to Heal Shame, the Inner Critic, Trauma and Attachment.
The Compassionate Mind
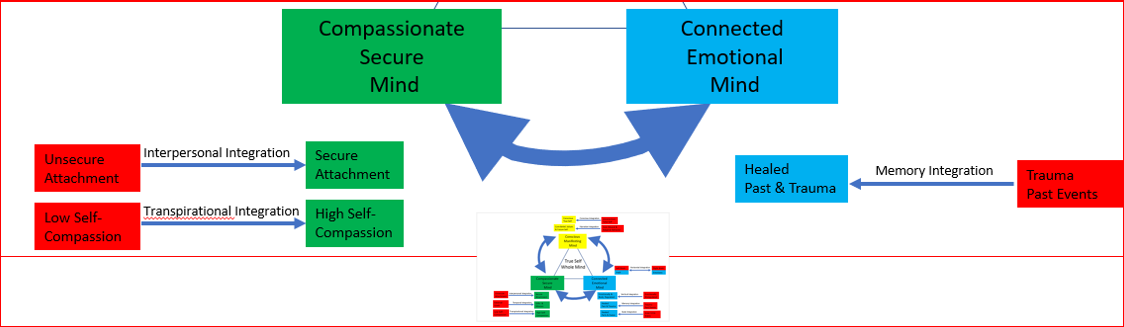
From the True Self Whole Mind Model, there are three parts to having a Compassionate Secure Mind:
Self-compassion
Secure Attachment Style
Gifts and Mission in how you lead yourself in the world.
In this article, we will discuss self-compassion and the secure attachment style in the context of healing trauma (development trauma) and healing the inner critic, both issues in the Connected Emotional Mind.
Self-Compassion and Attachment Styles Correlation
Self-compassion and attachment styles I have found are highly correlated based on my subjective experience. The science of attachment has shown that insecure attachment creates fears of positive social emotions like gratitude or connection. I have noticed that those who have a secure attachment normally score high in self-compassion. Those who score low on both can create an earned secure attachment by building high levels of self-compassion.
It is interesting to note that self-compassion appears to be good for a host of things: trauma, good relationships, and even help for chronic pain. Attachment is also good for a similar range of things because it appears a person when faced with life challenges can access the love or attachment from childhood. I have seen that those who have developed self-compassion eventually can have an earned secure attachment. And those that already have a secure attachment, often score high in self-compassion. See below for the tests to rate your self-compassion and attachment style.
Quiz for the Compassionate Mind
For your self-compassion score and attachment style, take these two free quizzes below.
Kristen Neff Self-Compassion (Statistically tested to be accurate) and 5 minutes for instant results.
https://self-compassion.org/test-how-self-compassionate-you-are/
Diane Poole Heller Attachment Style (Free, but not necessarily accurate—gives indications)
https://dianepooleheller.com/attachment-test/
An accurate attachment assessment needs to be done via a therapist who is skilled in attachments. However, I have found Diane’s test to be a good indication and it’s free and takes only 5 minutes. I noted that both no longer email the results, so take a screenshot of your test results.
Note that Kristen Neff's website also has several free meditations on self-compassion. I believe if you go through them for 6 weeks, 20+ minutes per day, you will increase your self-compassion.
Another person who has that nice self-compassionate, secure attachment tone is Rebecca Maclean, a Master RIM teacher. Her RIM-style meditations, 278 of them, are all public on YouTube.
https://youtube.com/playlist?list=PL98KTgOzjVw50RJ9jA0RWnNeY7pIRlyyq
People can also find her on Insight Timer, a meditation app.
What is Compassion
Many people associate compassion with niceness. However, it is much more than that. It involves making an effort to alleviate the suffering. Dr. Paul Gilbert, the inventor of Compassion Focused Therapy, notes a universal notion that compassion has two parts:
Sensitivity or awareness to suffering or pain in ourselves or others
Making an effort to alleviate that suffering
This two-part definition is also supported by the spiritual context. According to the Dalai Lama compassion is:
“Sensitivity to the causes of suffering in one’s self and others (Part 1), and the commitment to try to alleviate and prevent it (Part 2).” Dalai Lama
Neuroscience pretty much supports the two-part idea because compassion inhibits the fear circuitry in the brain (kindness) and leaves us ready to face difficulties (action).
Compassion is Motivation Also
This becomes very important because most people understand compassion to be only sensitivity to suffering or Part 1, and do not understand that it also involves the courage to not only feel the pain but also to do something about it or Part 2. Compassion is not only being nice, compassion is motivation or action also.
In the article the Benefits of Self-Compassion Dr. Andreas Comninos notes that compassion is the courage to do something (Part 2) and a set of skills (Part 1) that consist of:
“Having precise and sensitive awareness of suffering (Sensitivity)
Allowing ourselves to feel moved (Sympathy); having an ability to understand what is going on from different perspectives (Empathy)
Having an ability to tolerate distress (Distress Tolerance)
Having a Non-Judgemental attitude regarding what is going on (awareness of distress without “adding to it” or going to threat/protective strategies such as “shame about shame”, anger about anger”, or anxiety about anxiety, of self-criticism about self-criticism.)”.
As he explains, “Compassion requires being willing to understand the nature and causes of suffering while also being willing and courageous enough to come into contact with (vs avoiding) that suffering, so that we can actually do something to eliminate or prevent further harm in the best ways that we can.
Biggest Misunderstood Concept of Compassion
The biggest misunderstood concept of compassion and self-compassion is they miss that compassion is having the intention to be helpful because that is what is needed when we are suffering. It is not only sympathy that is a component of Part 1, but also the need for action. That action could be a) as simply as giving ourselves warmth or soothing OR b) taking action to remove the suffering using a loving strategy vs. threat or fear-based strategy.
Essentially Compassion is using the Soothing-Drive System (vs the Threat-Drive System).
The 3 Components to Self-Compassion
Kristen Neff, the best-known researcher in the USA on self-compassion and the person who elevated the practice of Mindful Self-Compassion, suggests that Self-Compassion has 3 major components:
Ability to recognize your pain and suffering and hold it in mindful awareness
Recognize that your struggles are part of being human and this is a shared aspect of common humanity
Treating yourself kindly.
A typical example is to bring awareness to the painful emotions and bodily sensations (could be your fear or anxiety or sadness) and responding with kind words and actions. For example: “It’s ok to feel this way, I know you are sad and your heartaches (perhaps you literally feel a pain in your chest). Place your hand on your chest to soothe the pain and bring warmth. It’s common for people (common humanity) to feel sad when they don’t succeed the first time. We will devise some actions to take. Devise actions and take them.”
Common Humanity
Self-compassion involves the first two parts of compassion 1) awareness or sensitivity to our suffering and 2) Taking Action AND adds a third component 3) Common Humanity—recognizing that this suffering is part of humanity.
So much of our suffering is not our fault. We didn’t choose our genders, our evolutionary brain, our families we were born into, the country, or our intergenerational and developmental traumas. So much has been determined externally to ourselves.
However, instead of blaming and shaming ourselves, we can courageously choose to take responsibility for our actions. Therefore, when are suffering, we can be aware of it and then take the action to do what is needed. This is self-compassion. Not just being nice.
Benefits of Self Compassion (from Benefits of Self-Compassion):
There are many benefits to self-compassion.
From: https://mi-psych.com.au/the-benefits-of-self-compassion/
1) It is one of the most powerful sources of coping and resilience.
2) Increases mindfulness
3) Reduces isolation
4) Anti-dote to the inner critic and the repercussions of a harsh self-criticism
5) Heals Shame and Anxiety
6) Heals Trauma and Attachment Wounds
7) Helps to deactivate the Threat System, so you are willing to make repairs in social situations and have more flexibility to deal with issues
8) More beneficial than self-esteem because it makes us more resilient, more caring, and less narcissism and reactive anger
9) Less fear of failing because you are able to support yourself after failure and therefore willing to try again.
10) More likely to succeed because there is less fear of success or fear of failure
Research has been shown the following:
1) Strongly predictive of well-being. People with self-compassion are more optimistic, more hopeful and have less anxiety, less depression, less shame, less suicidal ideation.
2) Almost same rewards as Self-Esteem, but less drawbacks. Self-esteem tends toward being better in comparison to other people and depends on achievement. Self-compassion is common humanity.
3) Linked to resilience coping. People who are kind to themselves are more resilient and bounce back faster from setbacks.
4) More compassion for others—when you are able to give yourself what you need, it increases your energy available to give to others. This also leads to less burnout.
5) Better relationships—people with self-compassion have better relationships. I have personally noticed that there is a high correlation between secure attachments and high self-compassion.
6) Compassion gives rise to positive emotions of gratitude and connection and reduces negative emotions like loneliness.
Myths of Self Compassion
1. Self-compassionate people are selfish
“For someone to develop genuine compassion towards others, first he or she must have a basis upon which to cultivate compassion, and that basis is the ability to connect to one’s own feelings and to care for one’s own welfare…caring for others requires caring for oneself.” Dalai Lama
“Teacher, which is the greatest commandment in the Law?” Jesus replied: “ ‘Love the Lord your God with all your heart and with all your soul and with all your mind.’ This is the first and greatest commandment. And the second is like it: ‘Love your neighbor as yourself.’ All the Law and the Prophets hang on these two commandments.” Matthew 22:36-40 NIV
As I like to say, you need to put on your oxygen mask first before you can save the baby. Both Jesus in Christianity and Dalai Lama, a current-day leader in Buddhism say that you need to love yourself as much as you love others. The Dalai Lama points out that learning to love yourself can be the basis of learning to love others.
2. Self-Compassion will decrease my motivation or lower my standards
People who are used to using their inner critic to motivate them using the Threat-Drive System misunderstand or do not know how to use the Soothing-Drive System. Both are effective in obtaining results. While the Threat-Drive System is great at obtaining results when there is high short-term danger such as a car is about to hit you (or a lion is going to eat you), the Soothing-Drive System of compassion enables you to access more options using your cortex and imagination which increases your probability of being successful in resolving relationship issues or more medium and long term issues.
You can access the Drive System without using the Threat System.
Furthermore, those who think compassion will just make them watch TV or play games instead of doing their work are confusing compassion with self-indulgence or self-pity. Self-indulgence is focused on your short-term pleasures, while self-pity is focused on being isolated (I am the ONLY person in the world who has this problem or yours is the worst in the world) vs common humanity (I am human and this is a human universal condition).
Self-Pity can also masquerade as self-hatred. By beating ourselves up, the inner critic (Threat System) may be trying to use shame and pain to motivate us.
3. Self-Compassion is a Weakness
Because self-pity or seeing a person “feeling sorry” for themselves (moping around with “bad luck”) is often confused with self-compassion, people see self-compassion as being weak. However, the contrary is true. Self-compassion is actually the antidote to shame and self-pity because self-compassion moves the person into a state of acceptance and feeling the difficult feelings (courage to feel the pain) AND then having the motivation to do something about the suffering. Self-compassion is actually a courageous act to feel the pain of suffering and wanting to do something to alleviate it.
Neurobiology of Self-Compassion
There are 4 ways that self-compassion can transform your neurobiology (especially when working with a coach or therapist):
1) Self-compassion inhibits fear and activates courage
2) Self-compassion shifts the brain neurology so that we can better handle our emotions and tolerate distress
3) Self-compassion changes the body via the vagus nerves and heart rate variability, which increases the resilience to stress.
4) Self-compassion improves mental health and psychosocial functioning.
Compassion Inhibits Fear and Activates Courage
Most people as noted think of compassion as niceness and a feeling of calm. In actual fact, compassion involves a feeling of stress and at the same time, the fear circuitry (Threat System) goes down, while the reward circuitry (Drive System) and caregiving circuitry (Soothing System) goes up. Compassion transforms an initial stress response into a caregiving or courageous response.
Neurobiology demonstrates that compassion is reducing fear and the courage to face and turn towards the pain of the suffering and the courage to take action whether that is just listening with compassion, or accepting the situation and be with that pain, or taking helpful action to alleviate the suffering.
There are 4 main parts of the brain that is involved with compassion: the insula, amygdala, the temporal-parietal junction (TPJ), and the pre-frontal cortex.
1. Insula
The insula which is part of the limbic brain picks up the signals of the bodily sensations that are experiencing sensations of pain or suffering, regardless of how the sensations occur—you could be reading, thinking, or seeing the suffering. Functional imaging experiments reveal that the insula has a role in pain experience and the experience of a number of basic emotions, including anger, fear, disgust, happiness, and sadness. The insula is essentially an alert system saying, “pay attention, suffering is happening”. The more we practice compassion, the more sensitive the insula becomes to picking up suffering.
2. Amygdala
The amygdala is an almond-shaped structure in the limbic brain. The amygdala is responsible for salience or “signaling this is important (or not)”. So the insula is saying hey, there is a signal going off in the body that something is happening. The amygdala determines if the signal is important and gets the body ready to act. Sometimes the amygdala can get the signal wrong and be oversensitive and overreact to the “threat”. So sometimes, we are overreacting to threats that might not be important.
3. Temporal-Parietal Junction
The temporal-parietal junction or temporoparietal junction (TPJ) is an area of the brain where the temporal and parietal lobes meet. Each side of your cortex (outer layer in the triune model) brain contains four lobes. The frontal lobe is important for cognitive functions. The parietal lobe is responsible for temperature, taste, touch, and movement, while the occipital lobe processes information about vision. The temporal lobe processes memories and integrates them with sensations of the 5 senses. The TPJ is responsible for taking the information from the senses and helps to decide about another person’s perspective. We are understanding another person’s point of view. “This person is suffering and can we help”.
4. The Prefrontal Cortex
The information from the insula, the amygdala, and the TPJ are then sent to the prefrontal cortex (PFC) for processing and decision making. The PFC makes appraisals of the situation and then decides what to do and how to do it. The PFC is saying “I feel there is suffering (insula), it is important and my body is ready (amygdala), and this is about another person and I believe it is important to help (TPJ)”. The PFC then processes: “I myself am not under threat and the person is not under threat, let me deactivate the Amygdala, or if it is self-compassion, the threat is a social threat, and I need to activate the Soothing System.”
Compassion Shifts the Brain’s Neurology
If the PFC decides to move towards self-compassion, the brain shifts from the Threat System and activates the Soothing-Drive System. The caregiver-nurturance pathway is located in the hypothalamic limbic system (mid-brain). The hypothalamus is responsible for homeostasis in the body. As previously noted, when we shift to the soothing system, oxytocin is released as the parasympathetic system comes online. The Drive System or reward system is also activated and provides dopamine for actions to help relieve the suffering (i.e. compassionate act). The Threat System is also deactivated, reducing the level of cortisol and adrenaline in the body.
We are therefore given pleasure (oxytocin) and rewards (dopamine) to be compassionate to ourselves and others. We are reinforced by nature to be kind to others and to ourselves and to help others.
Studies Demonstrate Compassion Shifts Can Be Learned
In the 2013 study Compassion Alters Altruism and Neural Responses to Suffering by Dr. Helen Weng and Dr. Richie Davidson at the University of Wisconsin-Madison, it was shown that a person only needed two weeks of 30 minutes per day of compassion meditation training (May you be healthy, May you be well to self, loved ones, relative, friend, and unfriendly) in order to be more altruistic and also modify the brains neurons in the parietal cortex (TPJ) and the prefrontal cortex (PFC). This was compared to a similar group given cognitive reappraisal training (cognitive behavior training by looking at the other person's perspectives, 1 year later, etc.). The increase in the PFC response downregulated the amygdala response for the compassion trained. So there was a biological change in the pathways and also a psychological compassionate response to moving towards others to help them (altruism).
This has also been shown over 6 weeks of training. In the 2012 paper Functional Neural Plasticity and Associated Changes in Positive Affect After Compassion Training by Oleg Klimecki et al, it was shown that compassionate meditation training can grow neural plasticity. This was one of the first studies to demonstrate neuroplasticity in the affective domain.
“The results suggest that compassion training can serve as a new, powerful method for enhancing positive affect in response to adverse situations. This is in accordance with findings of beneficial effects of compassion training for strengthening personal resources (Fredrickson et al. 2008) and health (Pace et al. 2009). As positive affect has been found to be associated with resilience (Fredrickson et al. 2003), future studies should explicitly address whether compassion training can serve as a buffer against stress, depression, and anxiety, and which physiological substrates mediate this effect.
Importantly, in comparison to other techniques for increasing positive affect, compassion benefits both, the person who experiences it (through strengthening positive affect) and the recipient of compassion (through fostering prosocial motivation). In the long-run, this promises to have major implications for the development of interventions for normal and clinical populations.”
We will show below how compassion can be used in interventions.
Compassion Increases Courage or Hope Circuitry
Note compassion increases the networks associated with caregiving and nurturing. These networks have also been called the courage or hope circuitry. It is amazing that in as little as 2 to 6 weeks of training our brain and behavior can be changed with compassionate training. The ability to widen our window of tolerance via compassionate training is very significant. It reduces our threat or anxiety responses and also opens our nurturing capacity to be more present and move towards caring for ourselves and others. This has been supported by neuroscience over the last decade.
Self-Compassion can train and build neural networks or neuroplasticity just as one builds muscles in the brain.
Compassion Shifts Sympathetic to Parasympathetic
Under the Polyvagal Theory, Stephen Porges postulated that the autonomic nervous system evolved in three steps:
1) Dorsal Vagal Complex – Freezing (Sharks and things without bones)
2) Sympathetic System – Fight or Flight system (Lizards)
3) Ventral Vagal Complex –Social Stimuli like Appease (Mammals)
With the Caretaking or Helping actions, oxytocin is released and there is a high vagal activation and a decrease in the heart rate.
Jennifer Stellar at the University of Toronto has done several studies with compassion and measuring the physiology of the activation of the parasympathetic nervous system (rest and digest) via the vagal nerves. She uses RSA (respiratory sinus arrhythmia) in her studies to measure vagal response. RSA is the naturally occurring variation in HR that occurs during the breathing cycle (our heart rate increases when we breathe in and falls when we breathe out). With compassionate activities, the parasympathetic nervous system is activated and our heart rate decreases. This corresponds to a downregulation of the threat system or sympathetic system.
Self-Compassion to Improve Mental Health
Using Self-Compassion to Heal Shame and the Inner Critic
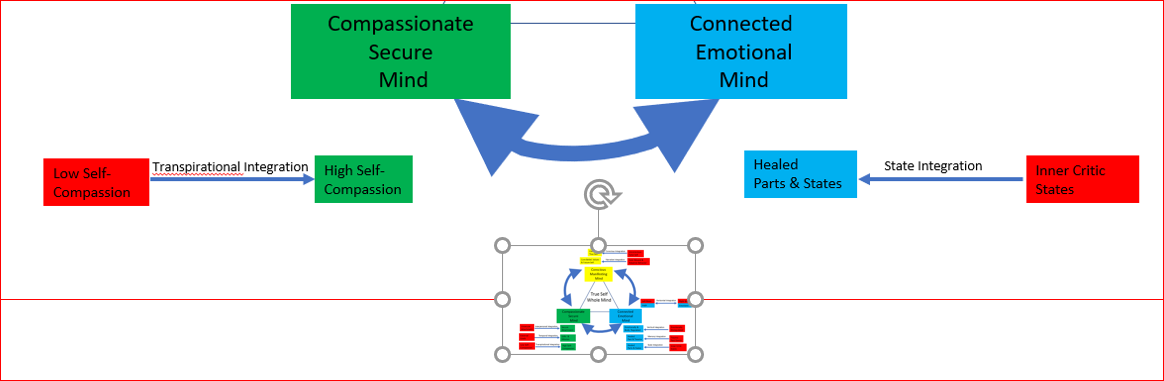
The above is a cut out of the True Self Whole Mind Model. In this next section, we will look at the interaction of how self-compassion can heal shame and the inner critic. I often find people who have low self-compassion will also have prominent inner critic and high levels of shame. The antidote is to increase self-compassion and once that is sufficient, use awareness and shift from the Threat System to the Soothing System to heal the shame and inner-critic.
Shame is an emotion. It is a safety warning. It is that bad feeling that we get when we feel we have done something to hurt the group or someone. It is the brain’s way of dealing with the threat of rejection or disconnection from a social group. We care how we are held in the minds of others and shame is a warning system that allows us to experience others as seeing us as somehow bad or wrong or inadequate.
Shame can show up physically in the form of hiding our faces (especially covered by your hand), blushing, fidgeting, or mumbling. Or it may come out as anger, withdrawal, or in the way we describe ourselves as foolish, defective, stupid, or lazy. Shame is often the glue that makes difficult emotions stick. You will normally find some element of shame hidden behind anxiety, anger, or grief. It is often the shame of “I am not good enough” or some variation of that.
Shame Cycle with Inner Critic
Shame is often associated with self-criticism by the inner critic. Shame often develops into a pernicious Shame Cycle. This makes shame really painful and difficult to dislodge from the psyche. First, there is the shame memory which makes you feel awful. We often move to a Threat System which triggers the inner critic. “You are a really bad person. You are really crap. You behaved badly. No one likes you.” And this makes things worse. The inner critic says all this in a threatening tone (i.e. fight response). This makes the shame-based memory even worse and it maintains the distress.
If you can’t tolerate the horrible shame state, then you may go to your safety strategy (drinking, drugs, food, or attack others) which can lead to further isolation. This often triggers more shame about the safety strategy and isolation, and other long-term issues with the safety strategy. The inner critic maintains and fans the flame of shame. Using self-compassion can disconnect the Threat System and inner critic which dismantle the shame cycle.
Shame is an Evolution Adaptation From Caveman Days
Shame is only fully developed in humans and is unique in humans. The human capacity for shame and related emotions of guilt or feelings of inadequacy, and social comparisons of wanting to be more than or feeling less than, etc. were probably formulated during human evolution from the caveman days. Chimpanzees, our nearest biological relatives, do experience minor forms of guilt and wanting to repair, but it’s nothing compared to humans.
So shame was developed by humans to help its evolution in a social context. Dr. Rick Hanson, the author of the Buddha’s Brain and NeuroDharma, explains that scientists believe that years ago hunter-gathers began to rely more on reputation and developed a way to punish freeloaders. Once there was a way to punish freeloaders and protect innocence and altruism, altruism grew along with other aspects of the social brain. If you were a liar or cheater, the social brain developed a capacity called “shame” or feeling ashamed, to make you know that you did something wrong socially, and you needed to make a repair or be kicked out of the group.
The development of shame was necessary so that the good parts of being altruistic and being collaborative could exist. Shame was a way of dealing with the freeloaders of this wonderful social system. If you did something to hurt the group, you would eventually be kicked out and isolation meant easy picking for lions.
3 Paradoxes of Shame
Keeping silent and hiding shame is what keeps shame alive. We are afraid that if anyone finds out, we’ll be rejected or shunned or found to be not good enough or defective. So what we do is isolate ourselves (the flight in fight or flight). And the anti-dote to isolating ourselves is self-compassion.
Many people are ashamed of being ashamed. In fact, when we can understand that shame is just an emotion and that is an evolutionary adaption to warn us, it makes it easier to deal with shame. These are the 3 paradoxes of shame.
1) Shame feels very blame-worthy, but it is just an innocent emotion.
2) Shame often feels isolating or separate, but it’s actually a universal emotion, everybody has it.
3) Shame feels as if it is encompassing, close to who we are, but it is actually a temporary emotion.
The Anti-dote to the 3 Paradoxes of Shame
In being compassionate, we can use the three parts of compassion to help remind ourselves of the paradoxes of shame.
First, we can mindful that shame is not who we are, it is temporary. Second, even though shame feels isolating, it’s universal and part of our common humanity. Third, shame feels blameworthy, but in fact, it is an innocent emotion, trying to be “kind” by helping warn us of a potential social threat.
The basic nature of people in other words is good. Sometimes in the shame, therapists will need to remind the client that their basic nature is good. Sometimes a person with self-hatred will think he is completely worthless and a piece of garbage. At these times, a therapist may ask before being harmed or being told these terrible things, if there was a time that “you wished to be loved”. Often the client will say yes because the wish was with the client since birth and the experience of not being loved was non-existent. Often the client will then choose to give himself and his inner child the love he never received.
3 Types of Shame: External, Internal, and Guilt
External shame is how we believe we exist in other people’s minds. It is the belief (often false) that if other people found out about who we really are, they would not like us because “I am not good enough” for the tribe or “I am defective” in some way or “I am not lovable or deserving of love”. These are often tied to our core wounds. These are painful and difficult experiences of shame. In working with external shame, a therapist may first want to offer validation and acceptance of the shame and try to find out what the client is hiding from by asking questions such as “What is your greatest fear” (often the response is that people won’t like me). The therapist can then have the client develop a compassionate orientation toward their external shame. External shame is often associated with social anxiety.
Internal shame is associated with what you think and feel about yourself to be true. Again these are feelings of “I am not good enough” and often associated with high levels of self-judgment. Internal shame can exist regardless of how well others perceive them. You can have both internal and external shame which is what happens in many depressed people.
Guilt is when we believe we have done something bad or wrong to someone along with the emotions of remorse or sadness AND the desire to repair it. The desire to repair it is an important aspect of guilt. You are not blaming or angry, you are sad that “I have done something to hurt someone” and you are thinking “how can I repair the damage of the hurt or relationship”. The person is not thinking about their status, or standing, or self-esteem, but on a caring behavior to help the person who was harmed.
Moving From External and Internal Shame to Guilt
Looking at caring behavior is also important when we work with ourselves. Often we are ashamed of hurting ourselves such as overeating or drinking, avoiding what needs to be done, spending too much money, wasting our day on social media, whatever we could feel ashamed about.
It is at these moments of shame, that we need to move away from shame and into guilt so that we can experience the sadness and sorrow and experience we are in a bad state and that we did that to ourselves without attacking ourselves. The feeling of sadness is the beginning of the change. We are able to grieve what’s happened and we can then feel “guilty”. Guilty is sadness AND wanting repair, so we can move into the caring mode of wanting to repair and then use self-compassion as the motivator to make the repair.
Using Soothing System Instead of Threat System
What we want to do is recognize that shame is a safety warning system. However, we often see the social threat as a physical threat. And we go into fight or flight (isolation). What we really need to do is use the Soothing System for repair, this is compassion (to repair things). We want to repair the situation to reconnect to the social group. We want to be in our social engagement system to repair or appease.
So when we do something wrong to the group or someone that is hurtful or unhelpful, we feel ashamed. What we want to do is move to a place of actually feeling guilty for hurting another, and then to say, “I’m so sorry I hurt you. I want to make things better. I want to make good on the hurt I caused you. I want to repair the damage caused by what I did (the thing I am ashamed of).
Because many of us have not developed a secure attachment and not developed a proper social engagement system, we have learned to use the Threat System to automatically respond to the shame danger. Rather than just accept it and listen and decide how to act, our Threat System is alerted and automatically goes into inner critic mode to respond. The inner critic uses the inner critic tools for fight (criticism or anger), flight (isolation and hide), or freeze (rumination), or fold (hopelessness).
Can you Handle the Social Threat i.e. It’s an Emotion, Window of Tolerance
One of the biggest lessons is to know what to do when a threat is there. We are naturally inclined to use our subconscious learnings and repeat our past patterns. When we can stop and breathe and be mindful, we are able to decide if we can handle the pain of the shame. Quite often the pain of the shame relates back to the past, at a time when we were very young and at that time we were unable to handle the pain and consequences of the shame and also the social threat.
When we are mindful and conscious, we can think if we can handle the consequences of the social threat. Often the answer as we grow older is yes. For example, when we were younger, being different and our unique self used to mean being ostracized for dancing differently. Today, as an adult, we can dance awkwardly or differently and if other adults don’t like our dancing, we know its no big deal, we know our true friends will not ostracize us. So we don’t need to worry about the shame or social warning. We can just keep dancing.
The important thing is to measure whether we have enough resources to handle threats. For example, when we have anxiety, our subconscious assessment is that the threat is greater than our resources. Then we have anxiety. When the threat is less than our resources, we don’t have anxiety. Our window of tolerance is wide. Similarly, when we have shame, is our window of tolerance, our resources, wide enough to tolerate that level of shame.
Just as importantly, when we were younger, we may not have been able to handle the pain if we were ostracized. We immediately flipped into the Threat System. Today, as adults we know if we breathe, we can handle more “shame pain” (our window of tolerance has widened) to be able to analyze the situation and then decide what we want to do about it. This enables us to shift into guilt and consciously have the courage to make the repair and say to another human being, “I’m so sorry that what I did hurt you.”.
Widening the Window of Tolerance
In widening our window of tolerance, we can use self-compassion to “soften, soothe, and allow”.
Soften the part of the body and allow the emotion. Perhaps putting the warmth of your hand on the part of your body that the emotion is located.
Soothe the emotion by talking softly to it from your heart (May you be well, or talking as a friend to it).
Allow the emotion is the mental aspect of allowing the emotion to exist as part of the human experience instead of clamping down on it and let it be there (feeling it a little, even if it feels bad).
Most likely the emotion will come and just pass through. “We give ourselves compassion not to feel better, but because we feel bad.” We are not trying to make the emotion go away.
Using Compassion In Therapy To Heal Shame
In working with pain or suffering, it is important to engage in both the head and the heart/body and the same goes for dealing with the pain of shame. In Buddhism, you need wisdom and love, the yin and yang to heal, two wings of a bird to fly. While either can be used to begin the work in therapy, neglecting one of these two will lead to trouble.
Many talk therapists will note that talking about shame almost feels irrational. Talking about the inner critic, telling ourselves we’re not so bad, telling ourselves that we should be nice to ourselves does not make us feel better. We need to connect to the inner hurt before we have the felt sense of feeling better.
Cognitively we can start to feel better when we understand what shame really is and that it is a human universal emotion. This tie to humanity is part of compassion.
In veterans returning from combat, self-compassion reduces suicidal ideation. Extreme shame can lead to thoughts of suicide. We can’t tell people to stop being ashamed because we know that doesn’t work. We can help people have compassion, kind of be understanding towards themselves and recognize that they aren’t alone and this reduces shame. Being kind and part of the human experience (i.e. the parts of compassion) and reduces things like PTSD and suicidal ideation. Using compassion to reduce the shame and self-criticism associated with PTSD reduces the level of PTSD and allows the mind to heal the remaining PTSD easier.
Therapy to Help You Learn 3 Things About Shame
In working with shame, a therapist is not trying to get rid of shame entirely, but to help you learn 3 things:
how to notice it,
what to do when it’s there,
how to recover from shame.
Once we notice shame, “oh that is my shame warning signal, that is my inner critic with a threat”, we can choose to switch to our developed compassionate mind and switch to our compassionate inner voice. We can notice the shame experience, watch it mindfully, perhaps go to a peaceful place or nurturing image (use imagery), and accept it with our breathing. We can then use our soothing voice to regulate back to what we want to do. See below for LALA+.
Compassion to Gain the Felt Sense of Care
We can use compassion to move towards the felt sense, the motivation to care, the felt sense of being loved. If for example, you are feeling terrible, like a piece of garbage. When we move into compassion, we disable the critic, and perhaps we can imagine a compassionate, caring, supportive presence who is on side of the “inner child”.
What would that feel like for you? What would that supportive person say? “It’s ok to not have finished your work today. Tomorrow, we’ll pick up back again. You are working hard. I’m going to be here for you. Yes, it’s hard and we will be able to get through it with more time.” It’s that loving presence. It’s felling that encouragement and when a person can feel that, they are able to have a felt sense that they don’t need to punish themselves.
The supportive compassion presence could be a relative, it could be an angel, it could be an animal, or even a character. Having a secure, nurturing, secure affective experience we learn what it is like to be in the presence of a caring person. Once we learn the “compassionate” experience, we can teach our higher self to speak to ourselves and provide us with the self-compassion to help with our shame. This is similar nowadays in sports, the coaches that are nurturing and encouraging yet with high standards are the ones having the best results.
The Core Belief in Shame
There is a mental component in Shame, a belief such as “I am not good enough”. There is also a physical component. While many therapists stick with the core negative belief and try to work with it, it is often faster to work with the physical component. In both RIM and Clear Beliefs, we will ask the client where they experience the shame in their bodies. This often leads to corrective experience with compassion. In Clear Beliefs and RIM, facilitators are able to use experiential experiences to clear the negative belief (Clear Beliefs) or rewrite the origin of the negative experience (RIM).
In naming the core negative belief with the client, a therapist would be compassionate with the client. “Oh really. I am so sorry. That must have been so hard. All that unnecessary suffering that you had to go through your whole life believing that”.
Compassion Focused Therapy and Shame
In Compassion-Focused Therapy, the goal is to help clients develop Compassion Motivation, the desire, and willingness to be really helpful.
Labeling the Shame Emotion
The very first thing to help heal shame is to label the emotion. Labeling the shame can deactivate the amygdala and move you out of reactivity into a place of perspective and imagination. LALA+ (Locate, Accept, Listen, Act) is a technique on how to handle emotions and helps to build emotional intelligence and fluency. In labeling, we are trying to help identify the sensations to recognize the shame (or emotion) such as the body heat, the increased heart rate, the uneasiness in the stomach, etc. Once we label, the sensations often reduce or become quieter. Label, quieter, label quieter almost as if to say: “hey do you hear me, I am feeling ashamed”(shame); “yes I hear you” (label); “are you sure you hear me, I am feeling bad” (shame quieter); “yes I am sure I hear “ (label).
Labeling on a neurological basis shifts where the flood is flowing. For most people when they don’t label, shame goes into the threat system because the person believes they are being judged and many will go into avoidance behavior. When you start labeling shame, it shifts the blood flow and creates a new neurological pathway that no longer overwhelms us. This begins the process of change. Then new skills like compassion can be used and eventually the client can build the confidence they can get out of the cycle of shame.
Once labeling is done, often it is easy to introduce the 3 paradoxes of shame, especially the aspect that shame is an innocent emotion and that everyone has shame. This is shame and the grass is green or the sky is blue. By labeling shame, it is being mindful and it validates the feeling and also brings them out of isolation.
Labeling is the equivalent of exposure therapy for our difficult emotions because we are often afraid of our shame emotions. Labeling also depersonalizes shame. It is the human condition, we feel shame because we are human not because we are bad. Shame does not heal shame. Threat-based minds don’t come up with insights that lead to recovery.
Also when labeling, remember it is important to not only name it but also the tone in which we are compassionate that we are experiencing the shame. The tone and energy we label the shame is important because the soothing tone activates the Soothing System.
In LALA+ the first thing is to Locate in the body the sensations (size, shape, color, etc) and when you can label these sensations, science has shown there is immediate relief of the pain or suffering. It’s as if the emotion has said, “o.k. you have acknowledged that I am sending you this danger signal that you are in danger of being kicked out of the tribe. “ We can then Accept this emotion by feeling it. Then Listen to what it has to say and then Act on it (hopefully you will choose to use the compassion system unless there is indeed a real threat).
Shifting from Shame to Guilt
Using the Threat System puts you into the overuse of the Threat Drive System. While the Threat System is good for saving us from extinction, it is not as good as the Soothing System, which uses the social engagement system for social issues. Shame is a social issue and what is needed ultimately is to use self-compassion to shift us out of the threat system of the Amygdala, and to move towards social engagement (the parasympathetic system) and the Soothing System. Then we are able to shift from Shame to Guilt (need for repair). This is a crucial step in shifting our emotions and also for healing Shame.
Once we understand that we have done something wrong to either another person or perhaps to ourselves and signaling to repair the situation (Guilt), we can feel the sadness of what occurred, soothe ourselves, and then using the social engagement system of turning towards others to repair or make amends of what we did incorrectly. By making repairs to the other person we can fix the social issue and we don’t “die by being isolated by the tribe”.
It is important to understand that some people can get triggered in therapy if they are already traumatized by someone who is nice and cheery (especially in facial gestures). So it’s important that in therapy, the delivery should be the right tempo (and tone).
We are shifting the intention and motivation. We are moving away from self-hatred and self-judgment, away from fear towards self-compassion and ultimately, what really matters is love.
Quieting the Inner Critic Using Wisdom and Love
In handling shame that is worsened by the inner critic, it has been noted that one cannot deal only with the shame via an argument with your mind. Shame will never be resolved without a felt sense in the body. However, quieting the inner critic is also a step.
One of the first things that can be done is in a compassionate way is to understand that the inner critic is not our enemy. The inner critic is trying to help us using the Threat System to fix something. So by listening to the inner critic, we can understand the situation better.
We can do what is known in Compassionate Focus Therapy as Functional Analysis. First, we can ask the critic what are the benefits of using the tools of the inner critic (anger, self-criticism, isolation, etc.). The inner critic will say that you won’t do that stupid dance anymore or you dress in more conservative clothes next time. What are the costs? You feel terrible about yourself, or you lose being who you are. Then finally, Is there another way to motivate yourself and still obtain the benefits without the costs (use self-compassion and shift from shame to guilt).
We can also bring levity to the situation. We can be thankful for the work our inner critic is doing. It may be really tired from having to work 24/7 to keep us safe and never having to miss a threat. Perhaps it wants to retire with all the other old critics or go away for a long holiday. Understanding that we are being the authors of our distress via criticism, we can also choose to recover. We ultimately are in control of our own minds.
Using Self-Compassion to Heal Trauma and Attachment Issues
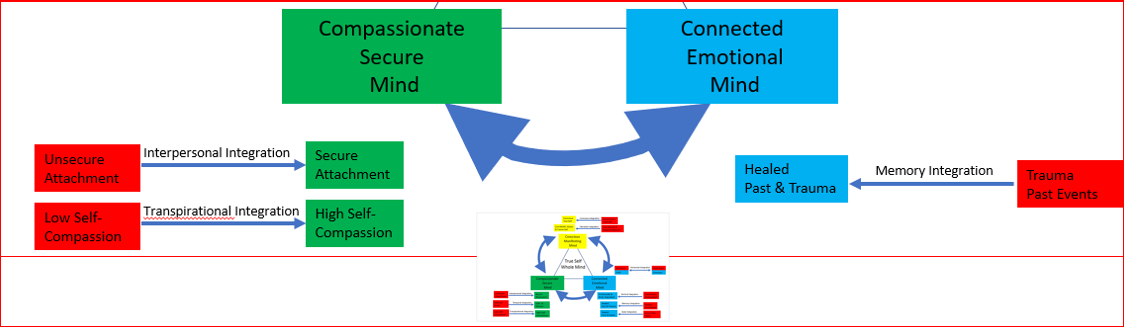
In this next section, we will look at self-compassion, secure attachments, and trauma. In the above diagram, you can see where these 3 components fit in the True Self Whole Mind System.
Self-compassion is normally impaired in those with developmental trauma and even PTSD. We have also seen that there appears to be a correlation between low self-compassion and insecure attachment styles.
Difficulty with Self-Compassion to Heal Trauma
Using self-compassion to heal developmental trauma or those with insecure attachments is made more difficult because the fundamental neural “train tracks” for self-compassion have either been covered up or not properly formed. This implies there needs to be more initial work to lay down the “train tracks” for self-compassion first before we can even begin to use self-compassion to heal trauma or an insecure attachment.
Early childhood experiences affect a person’s ability to practice self-compassion. Fortunately, self-compassion is a skill that can be learned.
Emotionally Nurtured the Basis of Self-Compassion
Compassion is normally learned from our mothers, our first teacher of compassion. We normally will receive caregiving from another. We will normally be clothed, fed, and educated AND we will be emotionally nurtured, which is the basis of self-compassion. So what if we do not have the emotional nurturance that nature provided for us as children, we need to obtain that attachment experience via a therapist (or another securely attached person) or through learning via self-compassion to be securely attached first before tackling our trauma via compassion.
While the skill can be learned, the trauma is normally made worse by the shame associated with trauma. A person with trauma will not have access to the Soothing System, so they are left only with the Threat-Drive System to deal with threats, even social threats that are best handled by the Soothing-Drive System with compassion. This normally creates excess avoidance, over control, self-harm, excessive addictions, and other interpersonal strategies that overwhelm the Threat System.
The Neurobiology of Attachment
As mammals, when we are under stress we will turn to our caregiver, who will give us a sense of comfort and safety hopefully. This will calm the nervous system and activate the soothing system which will give us oxytocin and endorphins. If a caregiver does not give us a sense of comfort, a child will feel less safe and threatened. This will activate the Threat System and increase cortisol and adrenaline.
In an insecure ambivalent attachment style, the child turned toward the caregiver and the response was ambivalent at best. The child learned an ambivalent attachment style. In adulthood, when things go wrong, an ambivalent attachment style grown child as an adult will not seek comfort through affiliation. With that adult, we can use self-compassion training as a kind of re-parenting program. Self-compassion then becomes about learning to find a safe haven or secure base within ourselves as adults. So when something goes wrong in adulthood, we can then turn towards ourselves with self-compassion and soothe ourselves via the Soothing System in the ways we were not as children.
Research has shown, that with angry faces, insecurely attached adults have a more robust amygdala response (Threat System) than securely attached adults. The insecurely attached person threat response is greater disrupted and disturbed. Therefore someone who learns to be self-compassionate to themselves and can have an earned secure attachment can train their neural circuits and pathways towards a more calm response.
Research from Kristin Neff and others has confirmed that we can re-parent ourselves and create an earned secure attachment. We are not trapped to relive continuously our early difficult childhood experiences. Like how we can train our bodies in the gym, we can train our minds for self-compassion.
How Self-Compassion Combats the Negative Effects of Trauma
As we have noted, people who have ruptured attachments resulting from trauma often are overusing their Threat System. They are hyper-aware of threats or have difficulty regulating their emotions and may experience high levels of anxiety, anger, sadness, shame, and self-criticism. Self-compassion can be used as an antidote to these high levels of experience by helping the trauma person move into the Soothing System and reduce shame and self-criticism. Self-compassion is often used in conjunction with other trauma-focused therapies such as EMDR or it’s incorporated into the therapy directly such as in Somatic Experiencing, NARM, or Compassionate Inquiry.
We will look in detail at how one kind of compassion-based therapy can be used to help heal Trauma. In Compassion Focused Therapy (CFT) the treatment of trauma is broken down into 3 steps:
Psychoeducation;
Compassionate mind training;
Bringing compassion to the traumatic memories.
Psychoeducation in CFT
In psychoeducation, the objective is to create the knowledge landscape so that people know they can have a way out of their pain. This is important because if you go immediately into the pain, it may really hurt and feel torturous and increases the risk that the client does not have a wide enough window of tolerance to soothe themselves. This may lead to self-harm or suicidal ideation or other unhelpful behaviors including quitting therapy. It’s therefore important that the client knows how to soothe themselves via self-compassion or other means.
It’s Not Your Fault
One of the important points in psychoeducation is to help clients understand that trauma, especially a ruptured attachment was not their fault nor is the resulting way they behave. Dr. Deborah Lee, a CFT therapist in a NICABM seminar notes,
…“three light bulbs “aha” moments that really resonate with my traumatized clients, one is a violation of human rights. It’s against the law to hurt and harm someone. And another is, “If the mind of the person who hurt you hadn’t existed, you wouldn’t have been hurt and harmed in this way. It’s not about you.” And the other really important bit about psychoeducation is traumatized minds make traumatized choices.” Dr. Deborah Lee
In other words, many adults blame themselves for the choices that they have made as adults in their relationships that hurt and harm themselves.” However, traumatized minds make neural circuits of traumatized patterns, which makes traumatized choices that are familiar versus choices that might have been better if the traumatized pattern was not there.
In CFT, it’s emphasized in a compassionate common humanity way that “it’s not your fault, you are not alone, and this is how we would all behave.” Notice also the use of “we” in compassion therapy, which helps to feel a commonality amongst humans. We would all be like that in those circumstances: “anyone who had this experience would of course react the way that you’re reacting.” In therapy, what we are doing is creating new neural circuits or patterns, so that the client can create new choices.
Fear-Based Responses in Ruptured Attachments
The natural response when one engages in a relationship is to be decent, open-hearted, and open-minded. However, for those with insecure attachment patterns from trauma (development or otherwise) such as anxious, avoidant, or disorganized attachments, the emotional expectation is that the person will be hurtful, critical, harmful, or rejecting. The relationship gets ruptured when the insecurely attached person gets triggered and goes into their safety strategy when triggered. It is as if an alarm gets triggered and the Threat System is activated that says “Safety, Safety, Safety”.
While the response might look different and complex, there are really only the basic strategies for safety: fight, flight, freeze, faint, or appease.
So in a relationship,
Fight = might be an aggressive or angry response.
Flight = might be the person walking out of the room.
Freeze or faint = might be someone just going silent and shutting out the other person.
Appease = might be to do something to appease the other person to make the “threat” go away.
However, these are all reactions that make the person disconnect from the relationship rather than connect in the relationship.
In Compassioned Focus Therapy the goal for ruptured attachment is to teach the person to shift to their compassionate mind and to engage in the relationship rather than go into the Threat System and engage in fight or flight etc. activities.
This understanding is very important to help those with developmental trauma begin to understand the effects that trauma has had on their lives and why their relationships are often damaged or they live in isolation. The Threat System allowed them to be “safe” but cost them the relationship. In the long run, using the Threat System instead of the Compassionate Mind is a losing strategy with original good intentions. Until they obtain this insight, the prefrontal lobe will not be able to switch strategies. So this psychoeducational step becomes the important first part of CFT therapy.
Developing the Compassionate Mind in CFT
The second step in handling trauma in CFT is to learn to feel what it feels to be really safe in a relationship. You need to learn to feel what you never felt before. You need to literally feel what it feels like to be psychologically safe. This requires you to train your brain and grow neurons that know how to engage in creating those felt sense of feeling compassionate and the inner voice of self-compassion (laying down or uncovering the train tracks of compassion).
It is therefore very important to learn compassion from a therapist or facilitator. This step or point is often overlooked. Self-compassion is not a read it and do-it-yourself book process. It takes mimicking someone with the right tone, right rhythm to learn from.
There are 4 components to CFT Compassionate Mind Training:
Mindfulness
The Perfect Nurturer
Breathing Exercises
Imagery such as a safe place like a nature (beautiful beach), faith (God or angel), or animal (pet)
The Perfect Nurturer is an interesting concept because this is very similar to the Dream House and Belief Closet in Clear Beliefs and also the Virtual Resource in RIM. The Perfect Nurturer would be non-judgment with perfect understanding, compassionate, wise, strong, and have the wisdom to find a way to get you unstuck or do something differently. There can be more than one Perfect Nurturer. We can even have an entire Caring Committee or Caring Army filled with these characters (how wonderful it is to draw from many characters.)
The Perfect Nurturer for Trauma Memories
In CFT, once the person has been able to develop a feeling of safety and is comfortable trusting this feeling of being safe, then the Perfect Nurturer can be brought into the compassion processing work associated with the trauma memories. This compassionate view allows the person to view the trauma from a distance in safety and not get caught back into the Threat System of the traumatic memories.
Traumatic memories are quite often unprocessed memories in the implicit memory bank instead of the explicit memory. Often, the person carries the unprocessed memories and draws incorrect conclusions and non-supporting beliefs. Flashbacks and nightmares represent unprocessed memories that seem happened in the past but appear to be happening now. These memories can be processed with a compassionate mind.
The compassionate mind also helps to increase the windows of tolerance, those enabling the client to engage longer in the processing of the traumatic memory.
Compassion is often used in conjunction with other memory reprocessing techniques such as EMDR, RIM, or Somatic Experiencing. It is important to not only have a mental understanding of the situation, but also a felt sense or body-emotional experience. Once the person has this felt sense of knowing, only then can the issue really be resolved.
The Felt Sense and Bodily Level
Quite often in trauma, there needs to be something that has to be done on a bodily level. For example, a person in a car accident might need to complete a movement—it might be as simple as taking off the seat belt and going out of the car to release the tension. Instead, they did not do this during the accident. When they replay the memory, they can see what needed to be done and are able to experience the motions.
At other times, they may know that they are not to be blamed, but do not have the felt sense and are still thinking the incident is their fault. When replaying the event with a more compassionate mind, they may be able to process a felt sense and understanding that they were only a child and that it was not their fault and what happened was the adult’s issue (e.g. inappropriate touching in childhood, where the child might have been convinced incorrectly it was their fault because they were a seductress of the adult at age 8).
Often in reprocessing, the person moves from shame to guilt (wanting to repair for the greater good) and then into action to resolve the hurt of themselves or others.
Judy Herman’s Model of Trauma
Judy Herman wrote a very well-known book called Trauma and Recovery. In her book, she explains a 3 part model to work with trauma:
Safety and Stabilization
Mourning and Re-processing the trauma memories
Connection and Integration.
In step one, this is similar to psychoeducation and creating the compassionate mind from CFT. Safety and developing resources are so very important. This is why it’s better to go to a therapist rather than a mindfulness teacher for trauma because the therapist will be able to create safety and ensure you develop the resources first.
Step 2 is similar to the processing of the trauma with the compassionate mind integrating other therapies. The compassionate mind can be supplied by the client or the therapist.
Studies are beginning to show that oxytocin is an important ingredient in creating better memories of traumatic events. Women who give childbirth have significant amounts of oxytocin released and despite the pain and trauma felt during childbirth, then often go on towards having more children. Ultra-endurance runners experience trauma and have significant amounts of oxytocin released and so they experience the events differently.
Memory Reconsolidation
There is a “warm glow” in memory reconsolidation, the ability to hold and process differently in the presence of a compassionate mind (therapist or your own). So compassion with the release of oxytocin plays a major role in transforming trauma.
In memory reconsolidation therapies such as coherence therapy, the therapist will guide the client towards disrupting the reconsolidation of the negative experience. If for example, the client expects that due to the trauma others will punish him or exile him. He will then expect that due to the violation, he will expect to be shameful.
If the therapist is compassionate and accepts him instead of the expectation of exile him, then the expectation of shame is disrupted. The person might feel that didn’t go as badly, or I was more capable, or I survived the experience and I am stronger than I expected. If skillfully handled, the memory will reconsolidate more favorably.
The Role of the Hippocampus in Trauma
In flashbacks, the hippocampus is not functioning properly. Often the person feels they are going to die. However, a different perspective can easily be brought by asking a question such as: “What does it feel like to you that you survived this experience?” (instead of thinking, “I feel I am dying”). The client may still feel shame from being degraded or violated in the trauma. In this case, chair work can be done. The flashback trauma would be in the center, and the chairs in the circle could be the feelings felt by our multiple selves such as disgust, fear, anger, shame, sadness, compassion. Often anger and sadness are not felt. The goal is to have these emotions expressed, especially focusing on the shift from shame to guilt (repair) to sadness. With compassion, sadness moves them out of the trauma and gets the client unstuck.
The Importance of the Compassionate Other
Many studies have shown that no matter the technique used for therapy, just having a compassionate therapist will produce significant results regardless of the therapy used. It seems that the compassionate therapist is more important to the therapy than the technique. Perhaps this is explained by the oxytocin created when people are socially bonded (such as even a talk about the trauma with a good friend).
Connection and Integration of Trauma
In Step 3 of Judy Herman’s Model, connection and integration, the person is integrating the insights from the previous 2 steps into their lives. Often, people will become social activists. Quite often, being no longer ashamed of their trauma and want to make other people’s lives better, people often do things to protect others from similar circumstances.
In the True Selves, Life Mission model, I often see this happening with my own clients who will then want to use their talents to help others. One person wanted to use yoga to help others deal with anxiety and stress and process trauma. Another wanted to teach teachers how to have more fun and bring themselves in the classroom more in alignment with their mission.
Backdraft Using Self-Compassion and Therapy
Backdraft is a firefighting term that happens when a fire has sucked out the oxygen out of the contained building and then reignites/explodes when a door is opened and lets in new oxygen. In psychotherapy, backdraft occurs when a person is not used to experiencing “compassion and love” and then suddenly is receiving compassion from the therapist and themselves.
One way to think about backdraft is that once you create a space for compassion, there will be a rush by the parts of you that needs love and compassion. The aspects of ourselves that need compassion will rush into that newly created space and those memories or traumas that were starved of affection will quickly rush into our awareness.
Backdraft in compassion can trigger old memories and trauma wounds. For example, a person who was sexually assaulted by a “kind and loving” relative. When they receive this kind and loving from the therapist or themselves, this might trigger the trauma; just as a traumatic smell re-experienced can trigger trauma. So opening your heart can actually be painful for some people.
With Backdraft in Compassion, one needs to go more slowly to introduce compassion. In some ways, when learning self-compassion it is important to titrate the experience. It is very similar to when you are exercising. You might feel sore etc. and eventually, you are able to tolerate more as you build your muscles.
Emotionally Opening and Emotionally Closing
There are also the key terms “emotionally opening” and “emotionally closing” to help clients address trauma. When dealing with clients, we can ask them if they are emotionally opening (aware, attentive, curiosity, the release of tears) or emotionally closing (tense, angry, tired). It is actually compassionate to yourself to close when it’s too painful. So allowing ourselves to close is ok. And another time, you can revisit the issue.
Fears, Blocks, and Resistance to Self-Compassion
Backdraft is one kind of fear of compassion that often comes up with fears associated with a caregiver with abuse. An analogy is people who felt sick after drinking a type of alcohol—for one of my friends, it was gin in university and I don’t think he ever touched gin again in university.
For resistance, one can use compassionate inquiry to explore further the reasons for the resistance. Often it may lie with one of the myths of self-compassion.
Blocks to self-compassion are often associated with the train tracks blocked or covered over. Exercises that focus on compassion skills training can be used to build self-compassion skills that can help us to respond with courage and care to threats.
C.A.R.E. Another Way to Heal Relationships Issues
Dr. Amy Banks in Four Ways to Click: Rewire Your Brain For Stronger More Rewarding Relationships has created a methodology to diagnose those with relationship issues and how each component relates to the 4 brain neuro-networks. She calls this program C.A.R.E.
A big premise of her work is that human relationships are important in the development of humans and relationships foster growth and health. This is in contrast to the boundary lead separation-independence theory that emphasizes human’s ability to stand independently as the ultimate end product of developmental growth. I prefer the RCT viewpoint and Dr. Bruce Perry’s book Born for Love is a good indication that RCT has neuroscience behind it.
Dr. Banks combines neuroscience and relational-cultural therapy (RCT) to outline the four benefits of a good relationship and the corresponding brain networks that need to be strengthened when we don’t have good relationships.
Calm: the pathways in the autonomic nervous system, specifically the vagus nerve (she calls it the smart vagus) from the Polyvagal Theory is in social engagement mode. i.e. safe.
Accepted: the dorsal anterior cingulate cortex or dACC is not highly activated. In Social Pain Overlap Theory, it has been shown those who feel left out triggers pain in the dACC which is very similar to real physical pain felt. You feel accepted and belonging, and treated as equals in the relationship.
Resonant: The feeling that other people “get” you. This is a result of our mirroring system working. When our mirror pathways are weak, it is hard for other people to read you.
Energetic: Energy is a benefit of the dopamine system. We, humans, receive pleasure in relationships, our energy levels are boosted from dopamine hits.
If you combine Calm and Energetic of CARE, you actually have Self-Compassion. If you combine Accepted and Resonant, you have Attachment Theory. So you will find the solutions are similar to someone using self-compassion to fix attachment theory i.e. you can shift into self-compassion to fix accepted and also energetic. What is nice about CARE is that you can see the individual components broken down.
I love the test of using your 5 main relationships (you are a product of your 5 main relationships some say) and seeing how you fare. It was an eye-opener for me (see my test below). The test identified why my relationships were giving me trouble and which people I could either avoid (i.e. were not calming for me) and which were not energizing me. You can do the test here for yourself.

The Various Kinds of Self-Compassion and Love
Just like the effects of meditation are similar for mindfulness, prayers, and mantras, the different names and process for compassion and love are very similar.
1. Self-Love
When I started my journey to consciousness, I learned how to love myself again or self-love from Anita Moorijani. She provide a meditation where I imagined a favorite grandmother or entity (Angel etc.) who would love you no matter what you did, even if you killed someone (and at that point, you would really need loving because you must have been in such a bad place in order to kill that person).
Once you were able to receive the love emanating from that favorite grandmother to you, no matter what you did, then you can transfer yourself into the image of the grandmother and send yourself this same loving energy and feel how it feels.
2. Self-Compassion/Compassion
We have written about self-compassion above.
3. Forgiveness
Forgiveness is a special form of compassion. It is reserved for the most difficult situations. For example, people you may dislike or for situations that are really difficult. We have also written about forgiveness in our Happiness Edition of Bamboo Newsletter #41.
4. Appreciation
Appreciation (Clear Beliefs) is a technique I learned from Lion Goodman of Clear Beliefs Institute. This is giving the person 50% of the loving feeling with your attention and then spending the other 50% in appreciation of the thoughts or actions of what they are doing or saying. This allows you to really understand with compassion why a person is like how they are (wow... it’s interesting due to the human brain and that person’s trauma how the brain responds with anxiety) and at the same time sending them loving energy (so channeling.
5. Reiki Energy
Reiki is a form of “channeling” universal energy. Essentially the person is imagining receiving energy from a universal source (love) and sending that energy via their mind or hands towards another individual. Therapeutic Touch and Prana Healing are using similar kinds of energy and concepts.
6. Gratitude
Gratitude is the ability to receive the love of the universe and to be grateful for the things around us, within us in the past, present and future. It’s related to the receiving and allowing of love. We have written an entire edition about Gratitude in Bamboo Newsletter #40.
7. Mindfulness, Meditation, Being Present
These are practices that have aspects of compassion, where mindfulness is one component of compassion.
8. Self-Care
When we care for ourselves via eating, exercising, sleeping, stress reduction, and other self-care activities, we are physically providing ourselves with loving actions towards ourselves. Entire practices are now also being rolled out for self-care.
9. Kindness
Kindness is the actions of a compassionate person to others and to themselves.
10. Loving Relationships
When we have loving relationships we are loving to others and providing the connection we require with others and allowing ourselves to receive love from others.
11. Work
When we do things to create things, we are both being kind to ourselves when we earn rewards such as money which can “self-care” ourselves financially.
Also when we are working with our mission in service to others, we are channeling our love into the work via our good deeds.
Action Items:
You have read this far. Give yourself a big hug.
Do the self-compassion and attachment style and CARE quiz.
Practice shifting from the Threat System to the Soothing System when you notice shame or your inner critic is responding to threats that require a compassionate response.